
Patient 1
0900:
Client is a 76-year-old man who was brought into the emergency department (ED) by rescue personnel, accompanied by his spouse. At 0800, his spouse found him on the floor of the bedroom. He was incontinent of urine, had slurred speech, and couldn’t stand due to paralysis in his right leg. Client is alert but unable to determine orientation because of global aphasia. Client’s grip strength in the left hand is adequate but is unable to grasp at all in the right hand. On the right side of the face, there is facial drooping. Client has a history of hypertension, diabetes, and atherosclerosis, according to his spouse. Spouse forgot to bring in client’s medication list but recalls he takes warfarin, “some type of statin,” metformin, and “two pills for his blood pressure.” Spouse reports client did not take any medication this morning.
Assessment findings:
- Cardiovascular: Atrial fibrillation with occasional premature ventricular contractions (PVCs). No murmur noted
- Respiratory: Tachypnea, lung fields clear
- Gastrointestinal: Positive bowel sounds
- Genitourinary: Incontinent of clear yellow urine
- Peripheral: Paralysis of right upper and lower extremity
| Laboratory Value | Result | Reference Range |
|---|---|---|
| Red blood cell (RBC) count | 4.7 million/µL | Male: 4.7 to 6.1 million/µLFemale: 4.2 to 5.4 million/µL |
| Hemoglobin (Hgb) | 14 g/dL | Male: 13.5 to 17.5 g/dLFemale: 12 to 16 g/dL |
| Hematocrit (Hct) | 45% | Male: 42% to 52%Female: 37% to 47% |
| White blood cell (WBC) count | 7000/mm3 | 5000 to 10,000/mm3 |
| Potassium | 3.6 mEq/L | 3.5 to 5.0 mEq/L |
| Sodium | 140 mmol/L | 136 to 145 mmol/L |
| Glucose (fasting) | 76 mg/dL | 65 to 99 mg/dL |
| Prothrombin time (PT) | 25 seconds | 11 to 25 seconds |
| Activated partial thromboplastin time (PTT) | 30 seconds | 25 to 35 seconds |
| Platelets | 350,000 µL | 150,000 to 400,000 µL |
| Blood urea nitrogen (BUN) | 18 mg/dL | 7 to 20 mg/dL |
| Creatinine | 0.8 mg/dL | Male: 0.6 to 1.2 mg/dL (53 to 106 µmol/L)Female: 0.5 to 1.1 mg/dL (44 to 97 µmol/L) |
0900:
Vital Signs – temperature 98.6°F (37°C), heart rate 120 beats per minute, respiratory rate 26 breaths per minute, blood pressure 180/98 mm Hg, and pulse oximetry reading of 93%
0915:
Noncontrast head computed tomography (CT) along with a CT angiography (CTA)
Rationale:
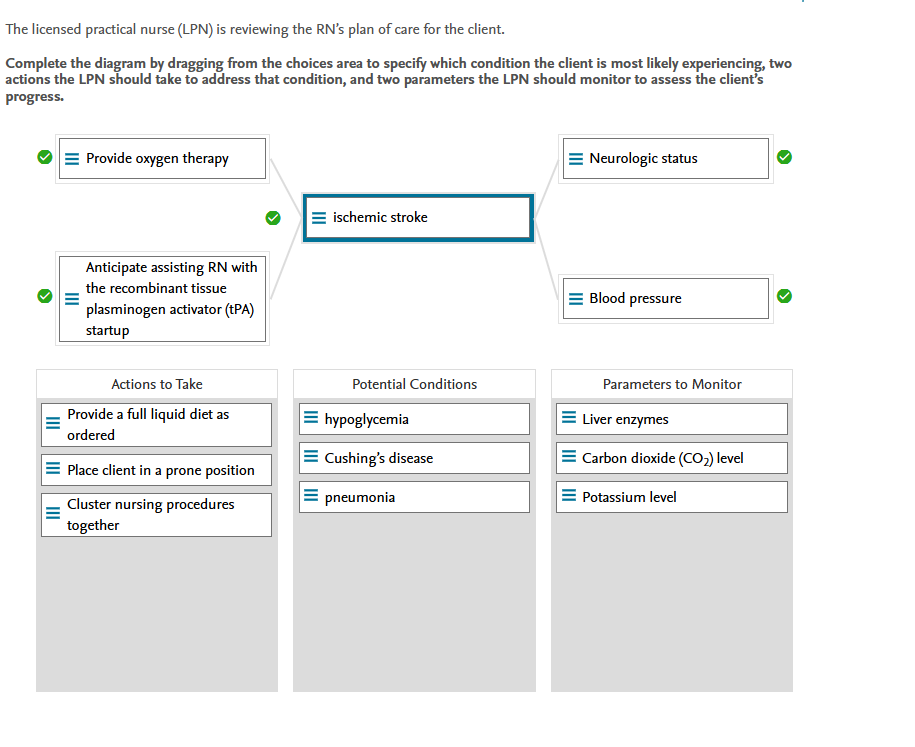
Potential Conditions:
Ischemic stroke occurs when blood flow to a part of the brain is interrupted by a thrombus or an embolus. Atrial fibrillation raises the chances of having an ischemic stroke. Other risk factors include hypertension, obesity, diabetes, a family history of the disease, and high cholesterol. A stroke manifests as one-sided weakness, unilateral droopiness of the face, slurred speech, difficulty swallowing, incontinence, tachycardia, and altered level of consciousness. The client’s blood glucose level was 76 mg/dL, which does not indicate hypoglycemia. Cushing disease is caused by a high cortisol level, which the client did not have. The client showed no signs and symptoms of a respiratory infection such as pneumonia.
Actions To Take:
Ischemic stroke treatment includes prompt assessment and diagnostic tests, followed by fibrinolytic therapy such as tPA. Any client with a pulse oximeter reading less than 95% should receive oxygen therapy. The client will not be allowed to eat or drink anything until he passes a swallow test performed by a speech therapist. The client will be placed in a position where the head of the bed is at least 30 degrees. To avoid an increase in intracranial pressure (ICP), the LPN should avoid clustering nursing procedures together.
Parameter To Monitor:
Fibrinolytic therapy, such as tPA, must be administered within 6 hours of the onset of stroke symptoms. While the client is on this medication, the LPN should closely monitor the client’s vital signs and neurologic status to see if there is any improvement or deterioration due to the stroke. Any changes in the client’s neurologic status must be monitored. During treatment, it is critical to keep the client’s blood pressure under control. It is not recommended that the LPN monitor the clients’ carbon dioxide, potassium, and liver enzyme levels.
10m 0s
Clinical Judgment Skill(s):
Recognize Cues, Analyze Cues, Prioritize Hypotheses, Generate Solutions, Take Actions, Evaluate Outcomes
Day of Admission 0800
Current height: 5 feet, 9 inches (175.3 cm)
Current weight: 230 pounds (104 kg)
Body mass index (BMI): 34 kg/m2
Vital Signs – temperature 98.4 °F (36.9 °C), heart rate 120 beats per minute, blood pressure 132/88 mm Hg, and oxygen saturation 93% on room air
Rationale:
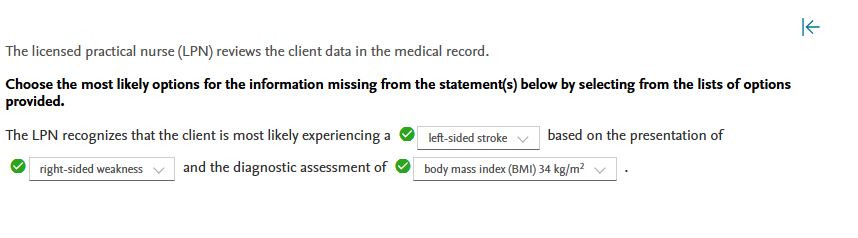
The client is most likely experiencing a left-sided stroke. Symptoms of a left-sided stroke include right-sided weakness or deficit, speech difficulty, and behavioral changes such as anxiety. The client is not suffering from a transient ischemic attack (TIA) because the symptoms persist. The client is not experiencing a right-sided stroke because the current deficit is on the right side. The confusion about time and place is consistent with stroke rather than delirium, which manifests as an acute onset of fever and confusion without other neurologic deficits. The client has a BMI of 34, indicating obesity. This is a risk factor for stroke. The client’s calcium and troponin levels are both normal. The client’s CO2 level is slightly elevated, which is most likely due to long-term heavy smoking.
1m 16s
Clinical Judgment Skill(s):
Recognize Cues
Day of Admission 0830
Chest X-ray: clear
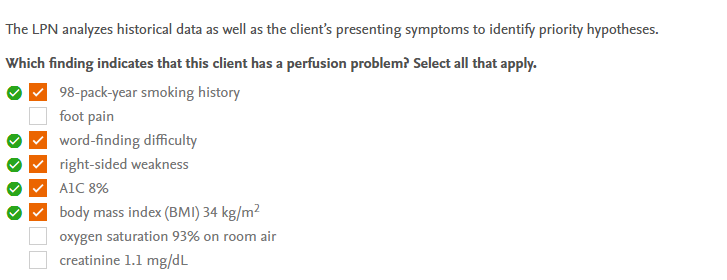
Rationale:
Stroke is caused by a lack of perfusion. A 98-pack-year smoking history is a major risk factor for stroke, affecting overall perfusion. Both word-finding difficulty and right-sided weakness indicate a decrease in brain perfusion. An A1C of 8% indicates that the client’s blood glucose is poorly controlled, which can affect perfusion and contribute to the development of stroke. A BMI of 34 kg/m2 is considered obese, and it is a significant risk factor for the development of changes in cardiovascular and neurovascular perfusion.
1m 23s
Clinical Judgment Skill(s):
Analyze Cues
Day of Admission 0945
- Admit to neurology unit for monitoring
Day of Admission 0830
Chest X-ray: clear
Day of Admission 0900
Computed tomography (CT) of head: positive for minor left ischemic stroke
Rationale:
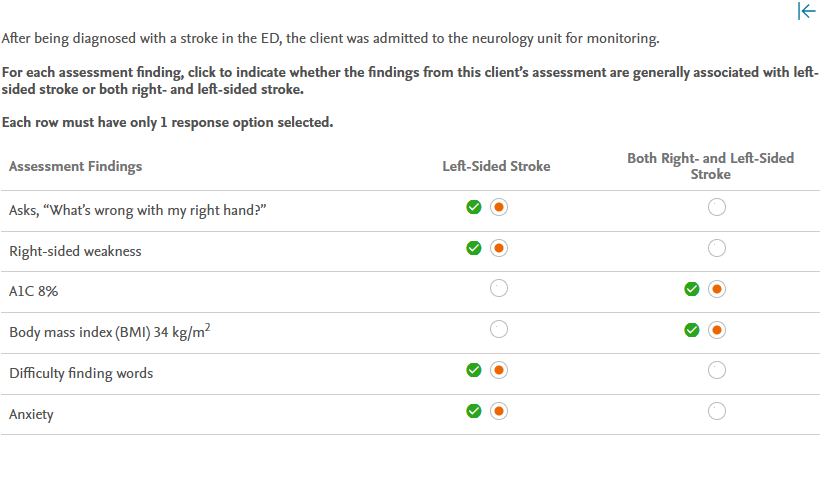
A left-sided stroke is characterized by weakness on the right side of the body, difficulty speaking, visual problems (particularly in the right field of vision), difficulty reasoning despite being aware of physical deficits, behavioral changes (e.g., depression or anxiety), difficulty reading, and memory problems. The client does not exhibit signs and symptoms of a right-sided stroke, such as weakness on the left side of the body, reduced insight (being unaware of deficits), visual problems (particularly in the left field of vision), depth perception challenges, inability to locate/identify body parts, memory difficulty, and behavioral changes (e.g., impulsivity, inappropriateness). The client has an elevated A1C, indicating poor glucose control, and an elevated BMI, indicating obesity, both of which are significant risk factors for any type of stroke.
1m 13s
Clinical Judgment Skill(s):
Prioritize Hypotheses
Admission
Initial client assessment and history completed. Client is oriented to person but is slightly confused about place and time. Client’s spouse and adult child are present at the bedside. The client requested a urinal and was able to urinate 60 mL of clear, yellow urine with some assistance holding the urinal. Client’s neurologic status remains unchanged, with decreased strength in his right arm and hand. Client is right-handed and unable to grasp items firmly with his right hand. A swallow study was performed at client’s bedside, and he was able to swallow thin liquids without difficulty. Gag reflex is intact. Client appears agitated, anxious, and has an elevated heart rate.
Day of Admission 0945
Admit to neurology unit for monitoring
Day of Admission 0830
Chest X-ray: clear
Day of Admission 0900
Computed tomography (CT) of head: positive for minor left ischemic stroke
Rationale:
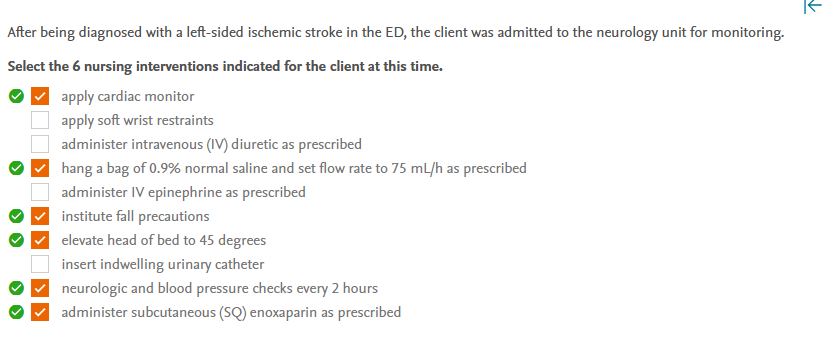
The LPN will prepare to intervene to support and maintain brain perfusion and oxygenation. This includes applying a cardiac monitor, performing neurologic checks and monitoring blood pressure frequently, supporting blood pressure with fluids, preventing venous thromboembolism (which can occur after a stroke) by administering enoxaparin, and elevating and maintaining the head of the bed at around 45 degrees to maintain appropriate intracranial pressure. Fall precautions are instituted because the stroke has affected the client’s strength and balance on the right side. Wrist restraints are not appropriate because the client is not displaying behaviors that endanger himself or others. There is no evidence that IV diuretics are necessary at this time; in fact, fluid balance is the goal rather than fluid removal. IV epinephrine is not indicated. The goal is to keep blood pressure within a normal range. The use of epinephrine causes an increase in the rate and force of cardiac contraction, resulting in an increase in cardiac output and blood pressure. Because the client can urinate successfully with assistance, an indwelling urinary catheter is not required. The insertion of a urinary catheter increases the risk of infection.
55s
Clinical Judgment Skill(s):
Generate Solutions
Admission:
Initial client assessment and history completed. Client is oriented to person but is slightly confused about place and time. Client’s spouse and adult child are present at the bedside. The client requested a urinal and was able to urinate 60 mL of clear, yellow urine with some assistance holding the urinal. Client’s neurologic status remains unchanged, with decreased strength in his right arm and hand. Client is right-handed and unable to grasp items firmly with his right hand. A swallow study was performed at client’s bedside, and he was able to swallow thin liquids without difficulty. Gag reflex is intact. Client appears agitated, anxious, and has an elevated heart rate.
Physical Assessment
- Alert and oriented to person and place; thinks the year is 2020
- PERRLA (pupils equal, round, reactive to light and accommodation)
- Tongue midline; no facial asymmetry noted
- Mucous membranes moist
- Heart rhythm regular with S1 and S2 present; no S3 or S4
- Capillary refill x2 seconds
- Anterior and posterior breath sounds equal bilaterally
- No cough
- No peripheral edema
- Abdomen soft and nontender; bowel sounds in four quadrants
- Upper extremities: strength on the right is +2 while strength on the left is +3
- Lower extremities: right +3, left +3
- One instance of word-finding difficulty noted (called tissues “sneezing paper”)
- Reports no pain anywhere other than the left hip, with a pain rating of 2 on a 0 to 10 scale
- Left hip with 3×3-inch contusion, greenish in color demonstrating healing process
- Feet warm and dry; pedal pulses strong bilaterally; nails thickened and light yellowish
Day of Discharge:
The client has been stabilized in the hospital for 72 hours with discharge home planned today. Symptoms of right-sided weakness continue to improve. Ambulating with assistance and feeding himself using his right hand. Discharge medications include: lovastatin (ongoing), amlodipine (ongoing), metformin (ongoing), aspirin (21 days), and clopidogrel (21 days). Smoking cessation materials given and referral to occupational therapy completed. Follow up scheduled with neurology and primary healthcare provider.
Day of Admission 0800
Current height: 5 feet, 9 inches (175.3 cm)
Current weight: 230 pounds (104 kg)
Body mass index (BMI): 34 kg/m2
Vital Signs – temperature 98.4 °F (36.9 °C), heart rate 120 beats per minute, blood pressure 132/88 mm Hg, and oxygen saturation 93% on room air
48 hours after admission
Vital Signs – temperature 98.8 °F (37.1 °C), heart rate 72 beats per minute, respiratory rate 18 breaths per minute, blood pressure 120/76 mm Hg, and oxygen saturation 94% on room air
Day of Admission 0945
Admit to neurology unit for monitoring
Day of Admission 0830
Chest X-ray: clear
Day of Admission 0900
Computed tomography (CT) of head: positive for minor left ischemic stroke
Rationale:
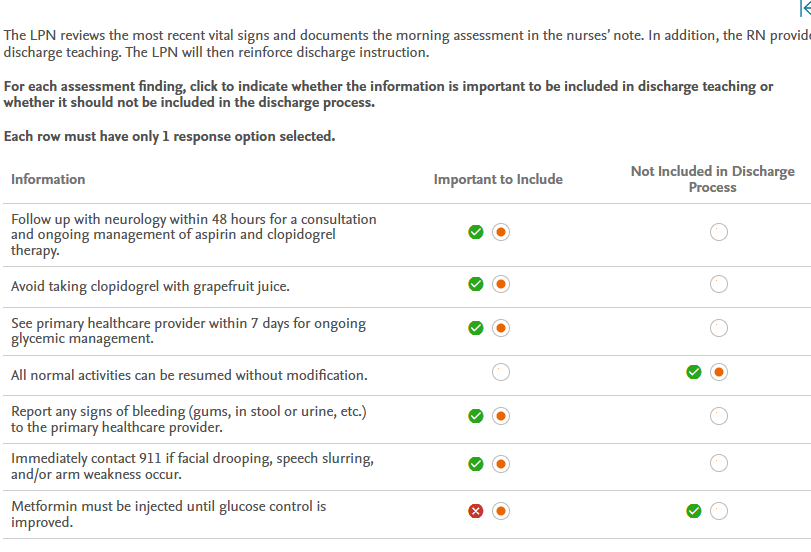
The client must be instructed to follow up with neurology within 48 hours for a consultation and to determine how to proceed with aspirin and clopidogrel after 21 days. Depending on the client’s ongoing risk factors, clopidogrel may be discontinued at that time or may need to continue. Aspirin is almost always continued after that time, with or without clopidogrel. Clopidogrel should not be taken with grapefruit juice because it interferes with the conversion of clopidogrel to its active form, decreasing the antiplatelet effect needed to prevent further strokes. To begin glycemic management, the client should see the primary healthcare provider. Bleeding of any kind should be reported right away because it can indicate that the client is not clotting properly. If symptoms of another stroke (facial drooping, speech slurring, and/or arm weakness) occur, 911 should be called right away to transport the client to emergency care. Because the client still has some weakness in the right upper extremity that will likely benefit from occupational therapy, normal activities should not be resumed immediately without modification. Metformin is prescribed orally, not by injection.
2m 10s
Clinical Judgment Skill(s):
Take Actions
Admission
Initial client assessment and history completed. Client is oriented to person but is slightly confused about place and time. Client’s spouse and adult child are present at the bedside. The client requested a urinal and was able to urinate 60 mL of clear, yellow urine with some assistance holding the urinal. Client’s neurologic status remains unchanged, with decreased strength in his right arm and hand. Client is right-handed and unable to grasp items firmly with his right hand. A swallow study was performed at client’s bedside, and he was able to swallow thin liquids without difficulty. Gag reflex is intact. Client appears agitated, anxious, and has an elevated heart rate
Physical Assessment
- Alert and oriented to person and place; thinks the year is 2020
- PERRLA (pupils equal, round, reactive to light and accommodation)
- Tongue midline; no facial asymmetry noted
- Mucous membranes moist
- Heart rhythm regular with S1 and S2 present; no S3 or S4
- Capillary refill x2 seconds
- Anterior and posterior breath sounds equal bilaterally
- No cough
- No peripheral edema
- Abdomen soft and nontender; bowel sounds in four quadrants
- Upper extremities: strength on the right is +2 while strength on the left is +3
- Lower extremities: right +3, left +3
- One instance of word-finding difficulty noted (called tissues “sneezing paper”)
- Reports no pain anywhere other than the left hip, with a pain rating of 2 on a 0 to 10 scale
- Left hip with 3×3-inch contusion, greenish in color demonstrating healing process
- Feet warm and dry; pedal pulses strong bilaterally; nails thickened and light yellowish
Day of Discharge
Client has been stabilized in the hospital for 72 hours and is scheduled to be discharged home. Symptoms of right-sided weakness continue to improve. Ambulating with assistance and feeding himself with his right hand. Discharge medications include lovastatin (ongoing), amlodipine (ongoing), metformin (ongoing), aspirin (21 days), and clopidogrel (21 days). Smoking cessation materials given and a referral to occupational therapy completed. Follow up scheduled with neurology and primary healthcare provider.
Physical Assessment
- Alert and oriented to person and place; thinks the year is 2020
- PERRLA (pupils equal, round, reactive to light and accommodation)
- Tongue midline; no facial asymmetry noted
- Heart rhythm regular with S1 and S2 present; no S3 or S4
- Capillary refill x 2 seconds
- Upper extremities: strength on the right is +2 while strength on the left is +3
- Lower extremities: right +3, left +3
- No instances of word-finding difficulty noted
- Feet warm and dry; pedal pulses strong bilaterally
Day of Admission 0800
Current height: 5 feet, 9 inches (175.3 cm)
Current weight: 230 pounds (104 kg)
Body mass index (BMI): 34 kg/m2
Vital Signs – temperature 98.4 °F (36.9 °C), heart rate 120 beats per minute, blood pressure 132/88 mm Hg, and oxygen saturation 93% on room air
48 hours after admission
Vital Signs – temperature 98.8 °F (37.1 °C), heart rate 72 beats per minute, respiratory rate 18 breaths per minute, blood pressure 120/76 mm Hg, and oxygen saturation 94% on room air
Before discharge
Vital Signs – temperature 98.8 °F (37.1 °C), heart rate 76 beats per minute, respiratory rate 18 breaths per minute, and blood pressure 120/72 mm Hg
Day of Admission 0945
Admit to neurology unit for monitoring
Day of Admission 0830
Chest x-ray: clear
Day of Admission 0900
Computed tomography (CT) of head: positive for minor left ischemic stroke
Rationale:
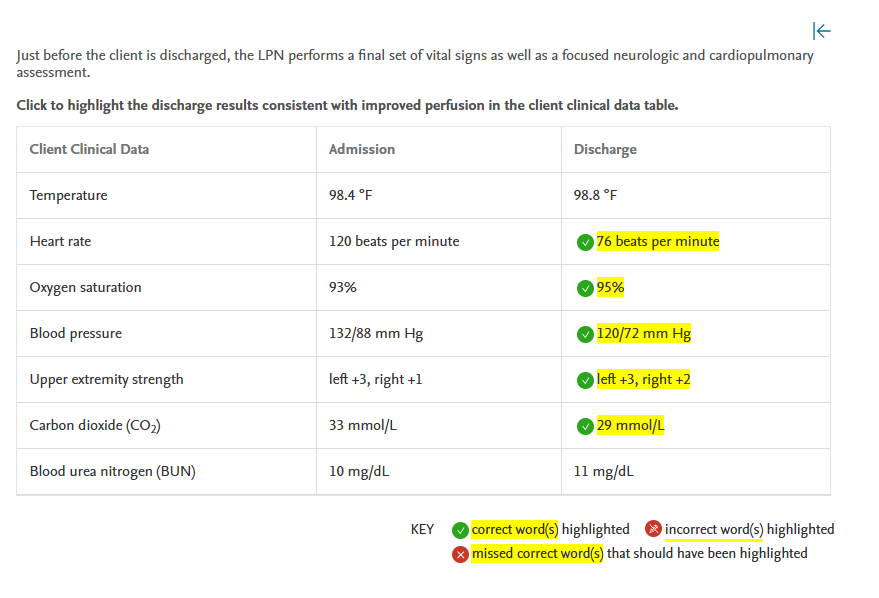
Changes in perfusion are associated with tachycardia, increased blood pressure, and impaired strength on one side of the body. Although the client’s slightly low oxygen saturation and slightly elevated carbon dioxide levels are most likely related to his smoking practice and history (and are likely always documented similarly), the improvement in these values during hospitalization also demonstrate an improvement in perfusion from baseline.
Assessment findings of a normal heart rate, improved oxygen saturation and CO2 level, normal blood pressure, and improvement in right upper extremity strength indicate that interventions have resulted in improved perfusion. The temperature within normal limits has no bearing on perfusion. The unchanged BUN does not indicate a change in perfusion.
2m 32s
Clinical Judgment Skill(s):
Evaluate Outcomes