
Hematologic – Patient 1
Patient Data
A 22-year-old African American man arrived at the emergency department (ED) with reports of excruciating pain in his back, chest, and lower extremities. Client is alert and oriented to person, place, and time. Family is at the bedside. Client’s skin tone appears grayish, and his sclera appears jaundiced. Client rates pain at a 10 out of 10 scale without any relief. Client is in tears and grimaces with every movement. Client is experiencing shortness of breath, nausea, and fatigue. He states that the pain has overwhelmed him and that he is unable to eat, sleep, or socialize with his friends. There is no prior medical history except for a broken femur from a football incident. Client states he recently returned from a two-week study abroad trip in China.
Assessment findings:
- Cardiovascular: Sinus tachycardia, no murmur noted
- Respiratory: Tachypnea, auscultated clear lung fields, dyspnea with mild exertion
- Gastrointestinal: Positive bowel sounds
- Genitourinary: Dark orange urine, episodes of urinary frequency and nocturia, denies burning or pain when urinating
- Peripheral: +1 pitting edema in bilateral lower extremities
done
That’s right!
Rationale:
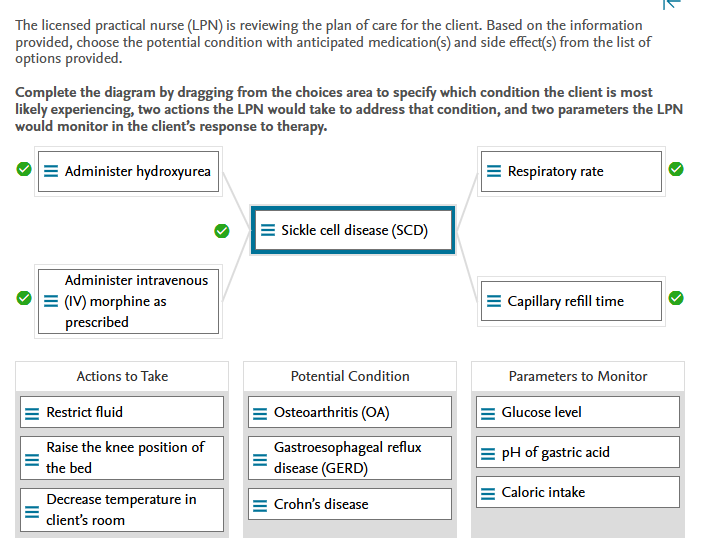
Potential Condition:
Sickle cell disease (SCD) is a genetic disorder in which the hemoglobin molecule in red blood cells (RBCs) is abnormal. This results in sickling of RBCs, which is often triggered by low oxygen levels in the blood. A sickle cell crisis could be triggered by high altitude, such as a long flight. Clinical manifestations include excruciating pain, anemia, elevated bilirubin, elevated white blood cell (WBC) count, tachycardia, tachypnea, edema, nausea, and shortness of breath (SOB). Osteoarthritis (OA) is an inflammatory condition caused by repeated damage to the cartilage in the joints. Clients with SCD experience joint pain, but this is due to the accumulation of sickled cells, which causes inflammation rather than cartilage damage. Gastroesophageal reflux disease (GERD) is caused by a backup of gastric acid, which causes damage to the esophageal lining. This causes heartburn and esophageal irritation. The client did not have any of the gastrointestinal (GI) symptoms associated with Crohn’s disease. This is a GI inflammatory disorder.
Actions To Take:
The LPN would anticipate administering hydroxyurea to the client, which would treat the sickle cell crisis by reducing sickled cells and increasing hemoglobin concentration. The LPN would also anticipate administering intravenous (IV) morphine to the client as prescribed. A common intervention is patient-controlled analgesia (PCA) with morphine. The LPN would encourage fluid intake rather than restrict it. The LPN would not raise the knee portion of the client’s bed because it could restrict blood flow to the joints. The LPN would also ensure that the room temperature is maintained at or above 72°F (22.2°C).
Parameters To Monitor:
Because respiratory depression is a side effect of morphine, the LPN will monitor the client’s respiratory rate. The LPN would also monitor the client’s capillary refill to ensure that there is no decrease in circulation, which would indicate circulatory compromise for the sickled cells. It would not be necessary for the LPN to monitor the glucose level, pH of the client’s gastric acid, or caloric intake.
Hematologic – Patient 2
Patient Data
Tuesday 1630 (admission to emergency department [ED])
A 38-year-old female client experienced loss of consciousness while shopping with her three young children at the grocery store. Client is currently awake and alert x3. Reports excessive fatigue and cold sensitivity. Heart monitor indicates sinus tachycardia. Client appears visibly pale and anxious.
Cardiac: Tachycardic; no audible murmur; no noted shortness of breath. Slight hypotension with orthostatic hypotension noted.
Eyes: Recent reports of blurry vision. Negative for scleral icterus.
Gastrointestinal: Client reports that she does not feel hungry and that the inside of her mouth is sore. Oral cavity reveals smooth, beefy red tongue and pale mucous membranes.
Respiratory: Tachypnea. Lung sounds clear to auscultation.
Neurologic: Report headache. No noted injury from the loss of consciousness.
Urinary: Reports some burning with urination.
Obstetric history: Three term births; zero premature births; zero abortions; three living children
Youngest child is 3 months old, uncomplicated vaginal delivery; currently breast feeding. History of heavy menses and endometriosis.
Social: Lives in a home with spouse and three children. Client is currently off work because of the recent birth; works as a financial advisor. Spouse currently at the bedside.
Tuesday 1630 (admission to ED):
Complete Blood Count (CBC) with Differential:
| Laboratory Parameter | Result | Reference Range |
|---|---|---|
| Hemoglobin (Hgb) | 7 g/dL | Females: 12 to 16 g/dL (7.4 to 9.9mmol/L)Males: 14 to 18 g/dL (8.7 to 11.2 mmol/L) |
| Hematocrit (Hct) | 21% | Females: 37% to 47% (0.37 to 0.47 volume fraction)Males: 42% to 52% (0.42 to 0.52 volume fraction) |
| Mean corpuscular volume (MCV) | 64 fL | 80 to 95 fL |
| Serum ferritin | 9 mcg/L | Female: 10 to 150 mcg/L (10 to 150 ng/mL)Male: 12 to 300 mcg/L (12 to 300 ng/mL) |
| Serum iron | 38 mcg/dL | Female: 60 to 160 mcg/dL (11 to 29 μmol/L)Male: 80 to 180 mcg/dL (14 to 32 μmol/L) |
Metabolic Panel:
| Laboratory Parameter | Result | Reference Range |
|---|---|---|
| Glucose (fasting) | 63 mg/dL | 70 to 115 mg/dL (<6.4 mmol/L) |
| Blood urea nitrogen (BUN) | 18 mg/ dL | 10 to 20 mg/dL (3.6 to 7.1 mmol/L) |
| Glomerular filtration rate (GFR) | 97 mL/min/1.73 m2 | >60 mL/min/1.73 m2 |
| Sodium | 140 mEq/L | 136 to 145 mEq/L (mmol/L) |
| Chloride | 96 mEq/L | 98 to 106 mEq/L (mmol/L) |
| Calcium | 9.4 mg/dL | 9.0 to 10.5 mg/dL (2.25 to 2.75 mmol/L) |
| Potassium | 4.9 mEq/L | 3.5 to 5.0 mEq/L (mmol/L) |
| Total Protein | 6.9 g/dL | 6.4 to 8.3 g/dL (64 to 83 g/L) |
| AST (SGOT) | 20 units/L | 0 to 35 units/L (0 to 0.58 μkat/L) |
| ALT (SGPT) | 19 IU/L | 4 to 36 IU/L (4 to 36 units/L) |
Urinalysis:
| Laboratory Parameter | Result | Reference Range |
|---|---|---|
| Color | Orange | Amber yellow |
| Clarity | Cloudy | Clear |
| Specific gravity | 1.015 | 1.005 to 1.030 |
| pH | 5.2 | 4.6 to 8.0 |
| Leukocytes | Positive | Negative |
| Nitrate | Positive | Negative |
| Protein | Negative | Negative |
| Glucose | Negative | Negative |
| Ketones | Trace | Negative |
| Urobilinogen | Normal | Normal |
| Bilirubin | Negative | Negative |
| Blood | Trace | Negative |
Tuesday 1630 (admission to emergency department [ED])
Vital Signs – heart rate 130 beats per minute, respiratory rate 28 breaths per minute, blood pressure 100/52 mm Hg, and oxygen saturation 92% on room air
Tuesday 1630 (admission to ED)
Chest X-ray: normal with no evidence of infiltrates
done
That’s right!
Rationale:
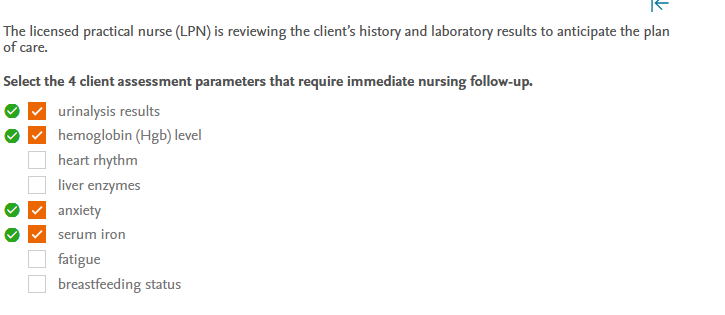
Urinalysis results, hemoglobin level, anxiety, and serum iron levels are the four client assessment parameters that necessitate immediate follow-up by the LPN. Because of the presence of leukocytes, nitrates, and blood in the urine, the results of the urinalysis indicate that a urine culture is required. All of these are signs of infection and relate to the client’s report of burning when urinating. The client’s hemoglobin and serum iron levels are critically low indicating a need for immediate follow up. Addressing the client’s anxiety is important. Her respiratory rate and heart rate are both elevated, and rising anxiety can complicate this. It is critical to ensure that the client is safe and well-cared for. While the client’s heart rate is fast, her heart rhythm is normal sinus. An increased heart rate is linked to both anxiety and laboratory values. The client’s liver enzymes are normal. The report of fatigue is consistent with the laboratory results. Current breastfeeding has no effect on client symptoms, there are no recommendations to change, and thus no immediate nursing follow-up is required.
Rationale:
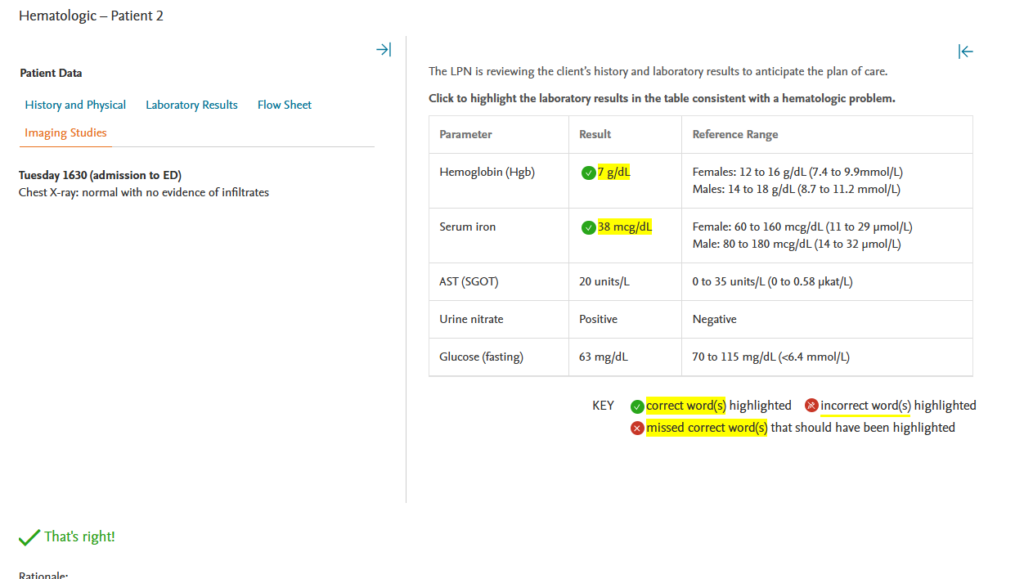
The very low hemoglobin value (7 g/dL) as well as the low serum iron level (38 mcg/dL) indicate a hematologic problem. The client’s liver enzymes are within normal limits. Although the urine nitrate and glucose levels are abnormal, they do not indicate a hematologic problem.
Rationale:
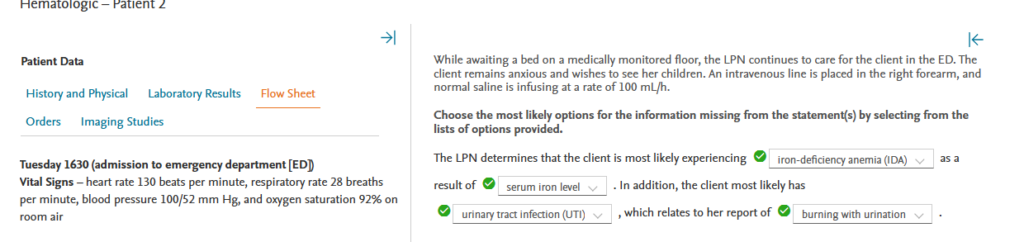
As a result of the serum iron level, the LPN determines that the client is most likely suffering from iron deficiency anemia (IDA). Aplastic anemia would result in leukopenia and a decrease in platelets, but this client has an elevated white blood cell (WBC) count and a normal platelet level. Polycythemia vera (PV) would result in elevated hemoglobin (Hgb) levels, and this client has low Hgb. Although sickle cell anemia (SCA) can result in an increase in white blood cell (WBC) levels, the presence of Hgb S is the primary indicator of SCA. The client most likely has a urinary tract infection (UTI), which relates to her report of burning with urination. The client shows no signs of gastroesophageal reflux disease (GERD). Decreased appetite, blurry vision, and fatigue are associated with iron-deficiency anemia (IDA). There is no evidence that the client has cataracts; however, the client’s anxiety is unrelated to the conditions presented in option 4.
Tuesday 1630:
- Insert intravenous (IV) line; begin 0.9% normal saline at 100 mL/h.
- Consult obstetrics/gynecology (OB/GYN) to evaluate for excessive menstrual bleeding.
- Consult with gastrointestinal (GI) to evaluate for potential GI source of bleeding.
- Type and crossmatch for blood administration; obtain consent for blood administration.
- Admit to medical monitoring floor.
Tuesday 1630 (admission to ED)
Chest X-ray: normal with no evidence of infiltrates
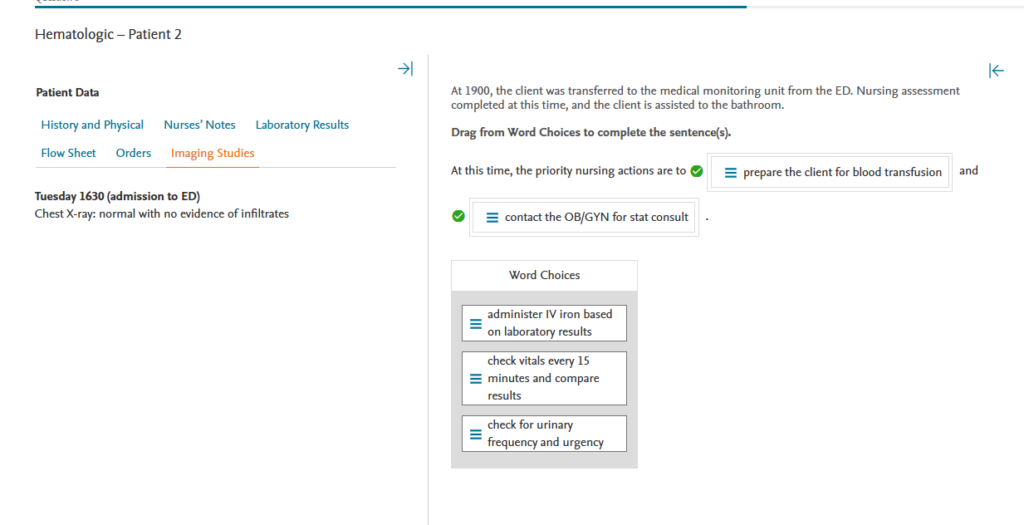
Rationale:
The priority nursing plan at this time is to prepare the client for a blood transfusion and to contact the OB/GYN for a stat consultation. The client’s hemoglobin (Hgb) and hematocrit (Hct) levels are critically low. Furthermore, the presence of large clots and excessive menstrual bleeding indicate that a gynecologic consult is needed quickly to determine the source of the bleeding. The LPN would not administer IV iron at this time. The priority is to improve the Hgb and Hct, which will in turn increase the iron level. As the client stabilizes, oral iron will be considered. Although it is important to monitor the client, checking vitals every 15 minutes is not warranted. The client is on a continuous heart monitor, and the priority at this time is to determine the source of bleeding and increase the Hgb. Urinary frequency and urgency are expected in the presence of a urinary tract infection (UTI). Even though the UTI requires attention, the blood loss remains the top priority.
Tuesday 1630:
- Insert intravenous (IV) line; begin 0.9% normal saline at 100 ml/h.
- Consult obstetrics/gynecology (OB/GYN) to evaluate for excessive menstrual bleeding.
- Consult with gastrointestinal (GI) to evaluate for potential GI source of bleeding.
- Type and crossmatch for blood administration; obtain consent for blood administration.
- Admit to medical monitoring floor.
Tuesday 1930:
- Infuse 2 units of packed red blood cells (PRBCs)
- Ultrasound of the abdomen and pelvis
- Transvaginal ultrasound
Wednesday 0800:
- Administer 200 mg of elemental iron PO
- Administer ascorbic acid, 1 tablet BID
- Repeat urinalysis
- Administer nitrofurantoin 100 mg BID, PO
The client received one unit of PRBCs at 2000 and the second unit at 2330. Ultrasound and transvaginal ultrasound completed. Currently in sinus rhythm with heart rate 88 beats per minute. Blood pressure is 120/64 mm Hg while sitting. Menstrual bleeding has decreased.
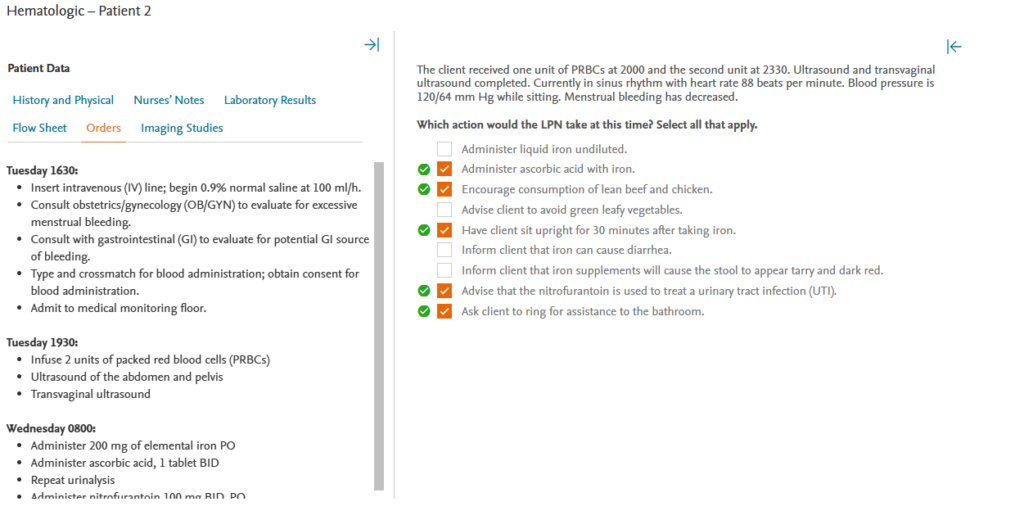
Rationale:
Because it can improve iron absorption, the LPN will combine ascorbic acid, also known as vitamin C, with the iron at this time. The LPN will also encourage the client to consume lean beef, chicken, enriched cereal and bread, as well as green leafy vegetables, to increase iron in the diet. Allowing the client to sit up for 30 minutes after taking iron can help reduce gastrointestinal (GI) side effects like heartburn. The LPN will explain to the client that nitrofurantoin is an antibiotic that is used to treat urinary tract infections (UTIs). The LPN will also ask the client to ring for bathroom assistance. Because the client still has low Hgb and Hct and has experienced orthostatic hypotension, assistance to the bathroom is critical for safety. The LPN will not administer undiluted liquid iron because it can stain the teeth. The LPN will inform the client that iron can cause constipation (rather than diarrhea) and turn the stool black (not tarry or dark red).
The client received one unit of PRBCs at 2000 and the second unit at 2330. Ultrasound and transvaginal ultrasound completed. Currently in sinus rhythm with heart rate 88 beats per minute. Blood pressure is 120/64 mm Hg while sitting. Menstrual bleeding has decreased.
For each assessment finding, click to indicate whether the interventions were effective (helped to meet expected outcomes) or ineffective (did not help to meet expected outcomes).
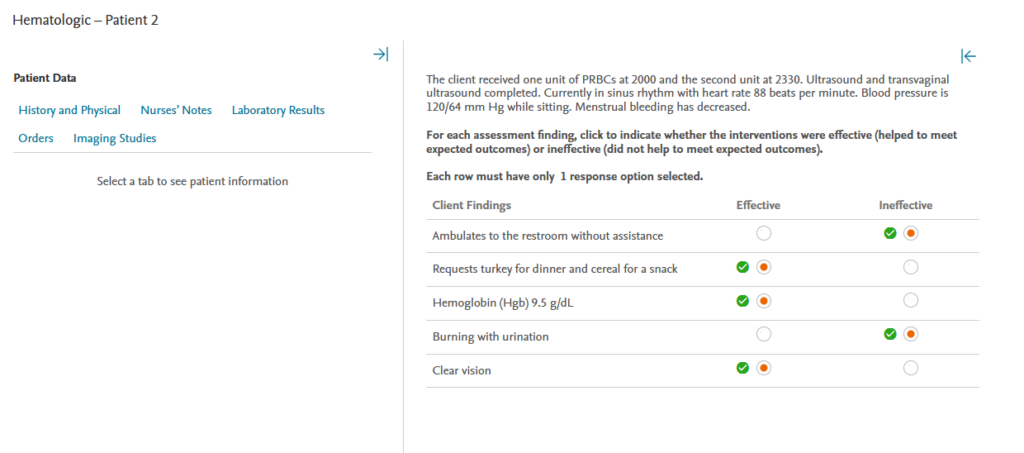
Rationale:
The client’s request for turkey and cereal indicates that she has received effective instruction regarding foods that can increase iron levels. Although the hemoglobin (Hgb) level is still low, it is rising, indicating that the interventions are effective. Because blurry vision is associated with severe anemia, clear vision indicates that the anemia is improving. The fact that the client was able to walk to the restroom without assistance indicates that the teaching to call for help was ineffective. The burning sensation when urinating indicates that the urinary tract infection (UTI) is still present and that the interventions have been ineffective.