
Cardiac – Patient 1
Patient Data
Client was brought to the emergency department (ED) by his son with reports of difficulty breathing and inability to walk short distances without becoming extremely short of breath. Client is a 72-year-old African American man who has a history of obesity, hypertension, coronary artery disease (CAD), and diabetes mellitus (DM). Client reports fatigue as a result of difficulty sleeping at night due to a nonproductive cough that has not been resolved with cough drops. Despite his decreased appetite, client reports a 10-pound weight gain in the past week. According to the son, his father has been unable to care for himself due to fatigue and increasing shortness of breath. He states, “he has not showered in over a week.”
| Laboratory Value | Result | Reference Range |
|---|---|---|
| Red blood cell (RBC) count | 4.7 million/µL | Male: 4.7 to 6.1 million/µLFemale: 4.2 to 5.4 million/µL |
| Hemoglobin (Hgb) | 12 g/dL | Male: 13.5 to 17.5 g/dLFemale: 12 to 16 g/dL |
| Hematocrit (Hct) | 40% | Male: 42% to 52%Female: 37% to 47% |
| White blood cell (WBC) count | 7000/mm3 | 5000 to 10,000/mm3 |
| Potassium | 3.6 mEq/L | 3.5 to 5.0 mEq/L |
| Brain-type natriuretic peptide (BNP) | 200 pg/mL | <100 pg/mL |
| Creatine kinase-MB (CK-MB) | 7% | <4% to 6% |
| C-reactive protein (CRP) | 5 mg/dL | Lowest risk: <1 mg/dLModerate risk: 1 to 3 mg/DlHigh risk: >3 mg/dL |
| Troponin | 0.7 ng/mL | <0.1 ng/mL |
| Cholesterol | 280 mg/dL | <200 mg/dL |
| Urinalysis | Positive for microalbuminuria | Negative |
Vital Signs at the ED – temperature 98.6°F (37°C), heart rate 120 beats per minute, respiratory rate 26 breaths per minute, blood pressure 152/90 mm Hg, pulse oximetry reading of 93%
- Electrocardiogram (ECG) reveals ventricular hypertrophy
- Chest X-ray reveals cardiomegaly
- Echocardiogram results pending
Assessment findings:
- Cardiovascular: Sinus tachycardia with occasional premature ventricular contractions (PVCs). No murmur noted
- Respiratory: Tachypnea, inspiratory crackles auscultated throughout bilateral lung fields, dyspnea with mild exertion, orthopnea, nonproductive chronic cough
- Gastrointestinal: Positive bowel sounds
- Genitourinary: Clear yellow urine, urinary frequency, and nocturia
- Peripheral: +4 pitting edema in bilateral lower extremities
done
That’s right!
Rationale:
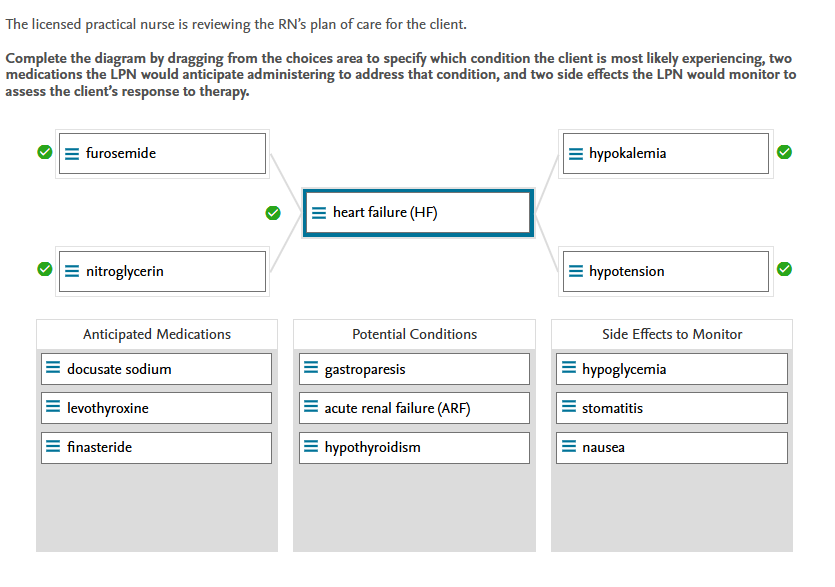
Potential Conditions:
Heart failure (HF) is a chronic condition in which the heart does not function properly as a pump. Tachycardia, orthopnea, fatigue, edema, fluid overload, and elevated BNP levels are all symptoms of this condition. Gastroparesis is a stomach complication caused by reduced stimulation and peristalsis. Acute renal failure (ARF) is a temporary loss of renal function that results in elevated serum waste products. Hypothyroidism is characterized by a decrease in thyroid hormone production, which leads to weight gain and muscle weakness.
Anticipated Medications:
Furosemide is a loop diuretic used to treat heart failure. Nitroglycerin is a vasodilator used to reduce the volume of blood returning to the heart. Docusate sodium is a stool softener used to treat constipation rather than HF. Levothyroxine is a thyroid hormone replacement therapy medication. Finasteride is a medication used to treat an enlarged prostate rather than HF.
Side Effects To Monitor:
Because potassium is lost in the urine when taking furosemide, the LPN should monitor for hypokalemia. Because nitroglycerin causes a drop in blood pressure, the LPN should keep an eye out for hypotension. Stomatitis are sores in the mouth that are frequently caused by chemotherapy treatment, not HF. There is no evidence that either furosemide or nitroglycerin cause nausea.
4m 31s
Clinical Judgment Skill(s):
Recognize Cues, Analyze Cues, Prioritize Hypotheses, Generate Solutions, Take Actions, Evaluate Outcomes
5 / 5 points
Cardiac – Patient 2
Patient Data
A 64-year-old male client has arrived for an outpatient clinic appointment due to difficulty breathing and a rash.
History:
- Hypertension
- Hypothyroidism
- Depression
- Erectile dysfunction
- Chronic back pain
- Hyperlipidemia
- Anterior wall myocardial infarction (MI) at the age of 44. Client had smoked two packs of cigarettes per day for the past 25 years, up until the MI. Client completed a cardiac rehabilitation program following his MI. His only physical activity at the moment is walking around at work.
Client reports sleeping on two pillows and waking up in the middle of the night one to two times per week, gasping for air and having to get up to urinate. Client has become more irritable and anxious. In the evenings, client experiences joint and back pain. When client walks more than 30 feet, he experiences increasing shortness of breath and is concerned about a red, scaly rash on his left lower leg.
Client’s body mass index (BMI) is 32 kg/m2. Client works as a manager in a retail clothing store. Client is divorced, with two adult children and a grandchild living in another state. Client lives on the second floor in an apartment.
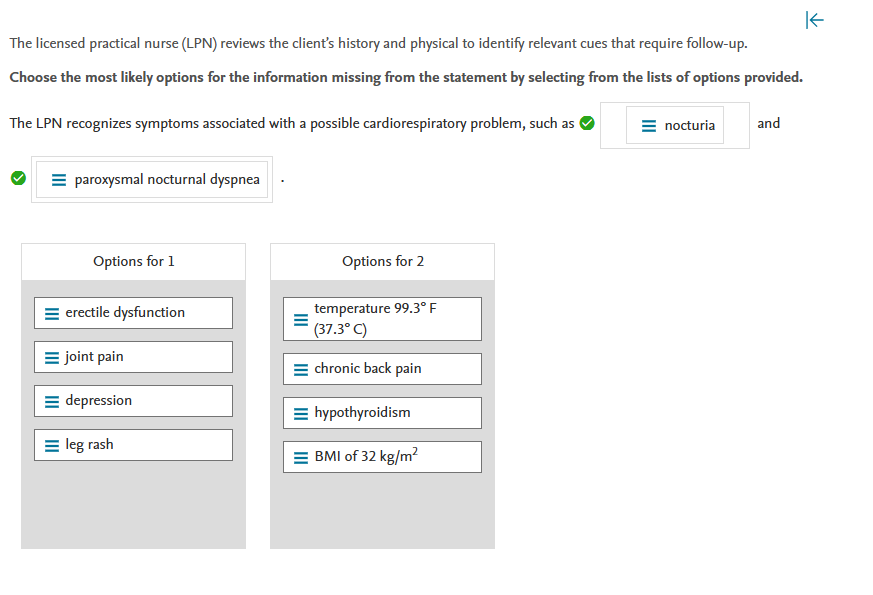
The licensed practical nurse (LPN) reviews the client’s history and physical to identify relevant cues that require follow-up.
Choose the most likely options for the information missing from the statement by selecting from the lists of options provided.
done
That’s right!
Rationale:
Nocturia (nighttime urination) and paroxysmal nocturnal dyspnea (waking up gasping with dyspnea) are two symptoms of cardiac dysfunction. Erectile dysfunction is frequently caused by a low testosterone level, rather than by a cardiac condition. Joint pain may be caused by inactivity or arthritis, rather than by a cardiac condition. Depression and leg rash are unlikely to be related to a cardiac condition. A BMI of 32 kg/m2 indicates obesity but is not a sign of a cardiac condition.
1m 11s
Clinical Judgment Skill(s):
Recognize Cues
1 / 1 points
Cardiac – Patient 2
Patient Data
1100:
Physical assessment performed:
- Client is alert and appears visibly anxious.
- Cardiac: Tachycardic; chest pain rated 6/10 scale; shortness of breath upon minimal exertion; hypertension noted.
- Eyes: Recent reports of blurry vision. Negative for scleral icterus.
- Gastrointestinal (GI): Active bowel sounds. Client reports that he is not hungry and has not eaten much in the past week.
- Respiratory: Tachypnea. Crackles auscultated in bilateral lower lobes.
- Neurologic: Headache reported. No loss of consciousness.
- Urinary: Client reports nocturia and clear yellow urine in adequate amounts.
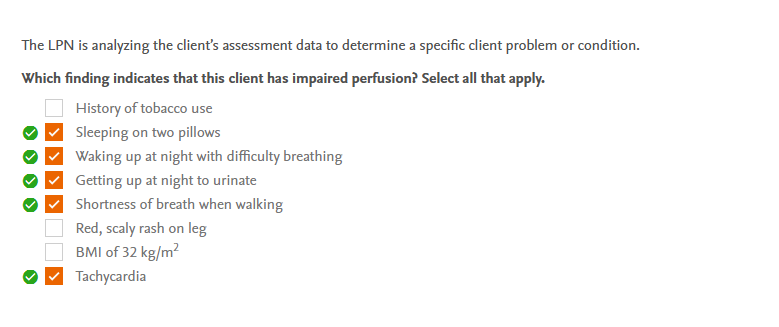
The LPN is analyzing the client’s assessment data to determine a specific client problem or condition.
Which finding indicates that this client has impaired perfusion? Select all that apply.
History of tobacco use
Correct answercheck_circle
Sleeping on two pillows
Correct answercheck_circle
Waking up at night with difficulty breathing
Correct answercheck_circle
Getting up at night to urinate
Correct answercheck_circle
Shortness of breath when walking
Red, scaly rash on leg
BMI of 32 kg/m2
Correct answercheck_circle
Tachycardia
done
That’s right!
Rationale:
Sleeping on two pillows, waking up in the middle of the night with difficulty breathing, and waking up in the middle of the night to urinate all indicate that the client’s heart is unable to manage fluid volume accumulated during the day. The heart is unable to effectively pump the increased volume as the client lies down and fluid is reabsorbed from the tissues into the vascular space. Shortness of breath while walking indicates an inability to meet the increased oxygen needs of the cardiac muscle. Tachycardia is a warning sign of heart failure and the body’s reaction to decreased cardiac output. Tobacco use may have contributed to the development of atherosclerosis, but there is no evidence of impaired perfusion. The rash is unrelated to cardiac output or perfusion, and it could be caused by a localized source of irritation.
43s
Clinical Judgment Skill(s):
Analyze Cues
5 / 5 points
Cardiac – Patient 2
Patient Data
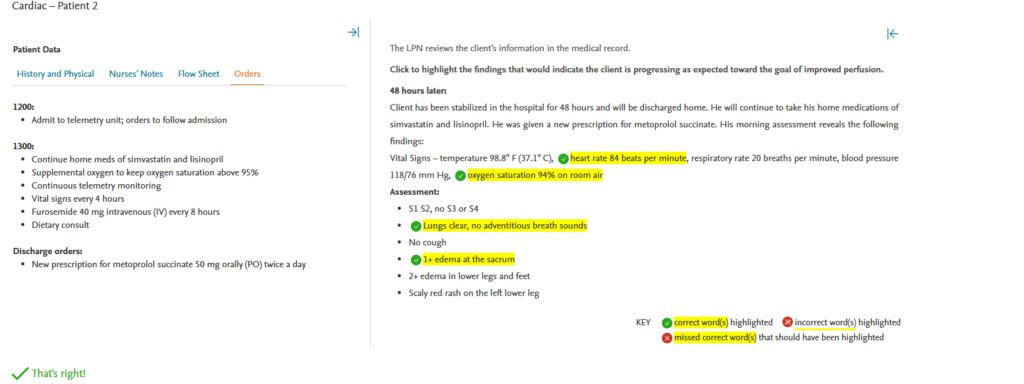
Current Vital Signs – temperature 99.3° F (37.3° C), heart rate 118 beats per minute, respiratory rate 30 breaths per minute, blood pressure 142/90 mm Hg, oxygen saturation 92% on room air
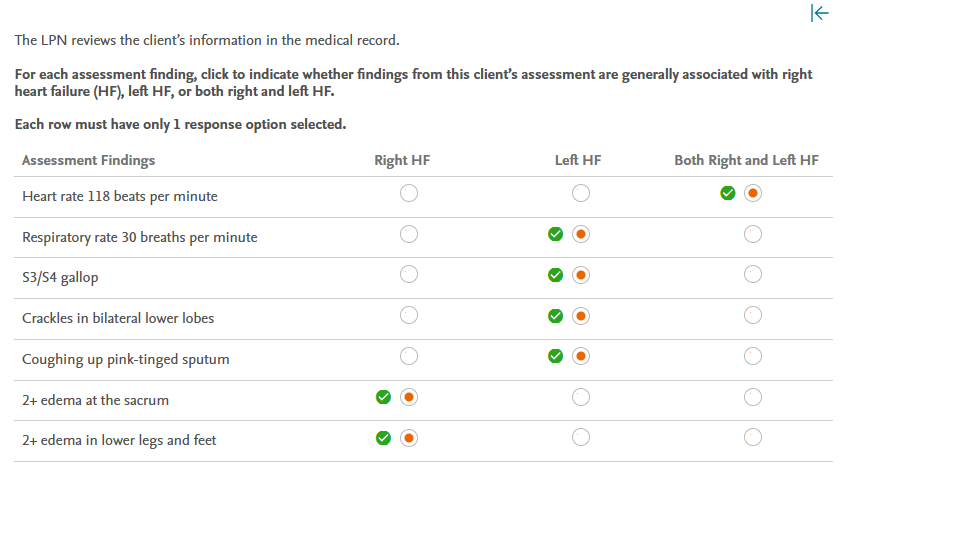
The LPN reviews the client’s information in the medical record.
For each assessment finding, click to indicate whether findings from this client’s assessment are generally associated with right heart failure (HF), left HF, or both right and left HF.
Each row must have only 1 response option selected.
Assessment Findings
Right HF
Left HF
Both Right and Left HF
Heart rate 118 beats per minute
Correct answercheck_circle
Respiratory rate 30 breaths per minute
Correct answercheck_circle
S3/S4 gallop
Correct answercheck_circle
Crackles in bilateral lower lobes
Correct answercheck_circle
Coughing up pink-tinged sputum
Correct answercheck_circle
2+ edema at the sacrum
Correct answercheck_circle
2+ edema in lower legs and feet
Correct answercheck_circle
done
That’s right!
Rationale:
Tachycardia is a compensatory mechanism in both right and left HF. Because blood backs up into the lungs with left HF, respiratory changes such as tachypnea, crackles, and pink frothy sputum are common. As blood backs up, right HF causes changes in the systemic circulation, such as in the extremities and gastrointestinal system. Edema develops in the dependent areas of the sacrum and legs.
1m 1s
Clinical Judgment Skill(s):
Prioritize Hypotheses
7 / 7 points
Cardiac – Patient 2
Patient Data
1200:
- Admit to telemetry unit; orders to follow admission
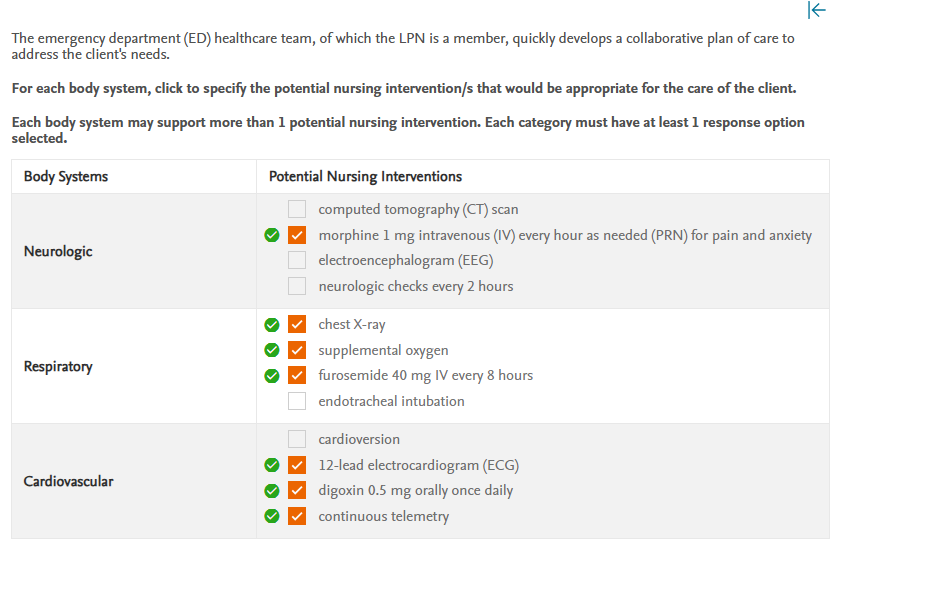
The emergency department (ED) healthcare team, of which the LPN is a member, quickly develops a collaborative plan of care to address the client’s needs.
For each body system, click to specify the potential nursing intervention/s that would be appropriate for the care of the client.
Each body system may support more than 1 potential nursing intervention. Each category must have at least 1 response option selected.
| Body Systems | Potential Nursing Interventions |
|---|---|
| Neurologic | computed tomography (CT) scanCorrect answercheck_circlemorphine 1 mg intravenous (IV) every hour as needed (PRN) for pain and anxietyelectroencephalogram (EEG)neurologic checks every 2 hours |
| Respiratory | Correct answercheck_circlechest X-rayCorrect answercheck_circlesupplemental oxygenCorrect answercheck_circlefurosemide 40 mg IV every 8 hoursendotracheal intubation |
| Cardiovascular | cardioversionCorrect answercheck_circle12-lead electrocardiogram (ECG)Correct answercheck_circledigoxin 0.5 mg orally once dailyCorrect answercheck_circlecontinuous telemetry |
done
That’s right!
Rationale:
The assessment findings indicate that the client is suffering from acute decompensated heart failure (HF). Collaborative interventions include providing supplemental oxygen, administering diuretics to treat fluid overload, and performing diagnostic tests such as a chest x-ray and 12-lead ECG to identify treatable problems that may be worsening the HF. Morphine would be given as needed to treat the chest pain and anxiety. The client would be placed on continuous telemetry to monitor for arrhythmias. Digoxin would be prescribed for a client with HF to alleviate cardiac symptoms. A CT scan would be performed to detect bone and joint problems rather than complications from HF. An EEG would measure brain activity, but it is not recommended for HF. If a client’s mental status changes, neurologic examinations are recommended. A client in respiratory failure would require an endotracheal intubation. Supplemental oxygen can be used to treat this client. A cardioversion would be recommended for a client who is in atrial fibrillation rather than tachycardia.
37s
Clinical Judgment Skill(s):
Generate Solutions
7 / 7 points
Cardiac – Patient 2
Patient Data
1200:
- Admit to telemetry unit; orders to follow admission
1300:
- Continue home meds of simvastatin and lisinopril
- Supplemental oxygen to keep oxygen saturation above 95%
- Continuous telemetry monitoring
- Vital signs every 4 hours
- Furosemide 40 mg intravenous (IV) every 8 hours
- Dietary consult
Discharge orders:
- New prescription for metoprolol succinate 50 mg orally (PO) twice a day.
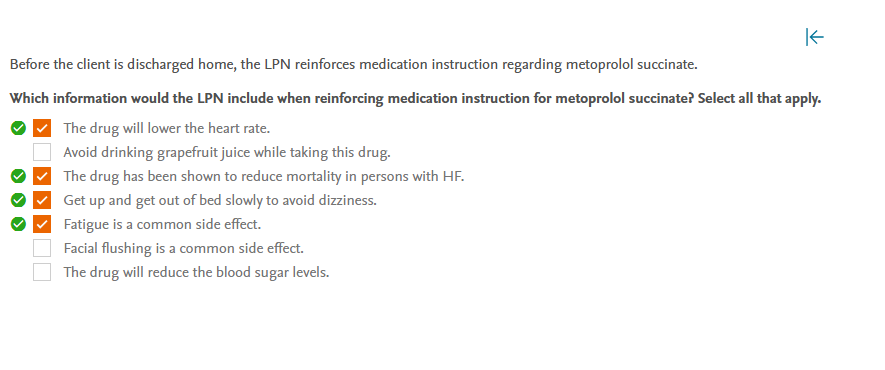
Before the client is discharged home, the LPN reinforces medication instruction regarding metoprolol succinate.
Which information would the LPN include when reinforcing medication instruction for metoprolol succinate? Select all that apply.
Correct answercheck_circle
The drug will lower the heart rate.
Avoid drinking grapefruit juice while taking this drug.
Correct answercheck_circle
The drug has been shown to reduce mortality in persons with HF.
Correct answercheck_circle
Get up and get out of bed slowly to avoid dizziness.
Correct answercheck_circle
Fatigue is a common side effect.
Facial flushing is a common side effect.
The drug will reduce the blood sugar levels.
done
That’s right!
Rationale:
Metoprolol is a beta-adrenergic blocker. The drug reduces heart rate and systemic vascular resistance, making it easier for the heart to empty blood into the aorta and lowering blood pressure. Because of the decreased resistance and blood pressure, the client may feel dizzy or lightheaded upon rising, which is a safety concern because it may contribute to falls. Beta blockers have been shown in studies to reduce mortality in clients with HF. Clients who start taking beta blockers frequently complain of extreme fatigue, which may or may not go away over time. Metoprolol can be combined with grapefruit juice; however, some statins and calcium channel blockers can reach dangerously high levels when combined with grapefruit juice. Metoprolol does not cause facial flushing; however, nitrate drugs and niacin frequently do. Metoprolol masks hypoglycemia symptoms but does not lower blood glucose levels.
6m 56s
Clinical Judgment Skill(s):
Take Actions
4 / 4 points
Cardiac – Patient 2
Patient Data
1200:
- Admit to telemetry unit; orders to follow admission
1300:
- Continue home meds of simvastatin and lisinopril
- Supplemental oxygen to keep oxygen saturation above 95%
- Continuous telemetry monitoring
- Vital signs every 4 hours
- Furosemide 40 mg intravenous (IV) every 8 hours
- Dietary consult
Discharge orders:
- New prescription for metoprolol succinate 50 mg orally (PO) twice a day
done
That’s right!
Rationale:
Tachycardia, low oxygen saturation, edema, and the presence of crackles are all signs of impaired perfusion in HF. The assessment findings of a normal heart rate, normal oxygen saturation, decreased edema, and resolution of crackles indicate that the collaborative interventions resulted in improved perfusion. The normal body temperature and the unchanged skin rash are unrelated and do not indicate a change in perfusion.
56s
Clinical Judgment Skill(s):
Evaluate Outcomes